Introduction
Over the past decade, the United States (U.S.) and its healthcare system have been criticized at the international level, arguing that it is one of the most financially secured countries but fails to deliver on providing adequate comprehensive cost-effective care for all of its people. Although this argument is valid for some, others disagree. U.S. healthcare is being targeted unfairly because the criteria for which the country is being evaluated on does not fair better than the richest countries in the world. Arguments can be made, but without knowing the entire situation and the healthcare criteria metrics of the country, critics need to step back and first learn, and attempt to fully understand, why the U.S. not only spends a lot of money on healthcare but also why many times the outcome from the delivery of healthcare has poor results. This paper will not only explain the unique nature of the U.S. in an effort to show why it is perceived by others that it is underperforming in the delivery of medical care, but will also discuss the quality of healthcare deliverance in the U.S. and how preventative health is given.
Setting the Stage: How Uniqueness of U.S.
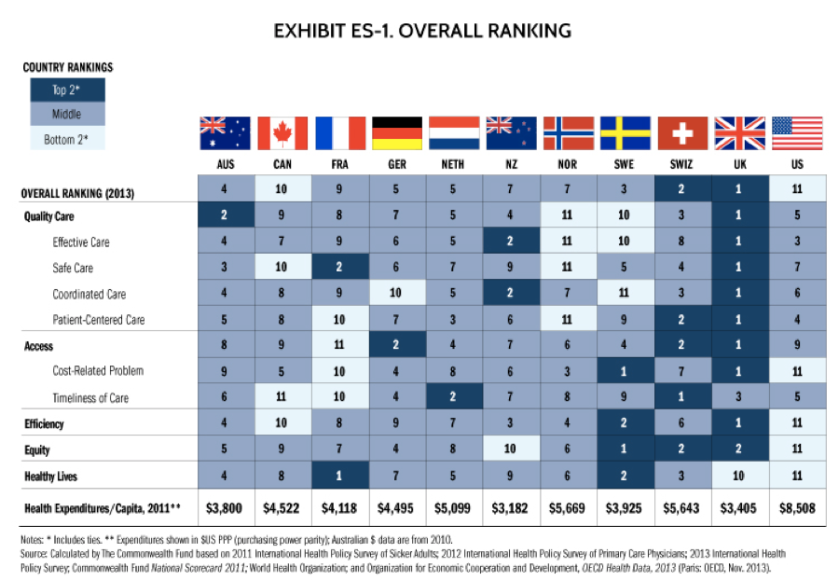
Anyone creating an argument can sound as though his or her opinion is more just and logical than that of any other. When arguing about the U.S. healthcare and how it compares to the rest of the world, one must first learn what makes the U.S. different from the rest of the other countries to which it is being compared. The U.S. is being compared with the top richest countries in the world in the category of healthcare. Currently the following countries are ranked based on the quality of healthcare from 1 to 10, respectively: United Kingdom, Switzerland, Sweden, Australia, Germany, Netherlands, New Zealand, Norway, France, and Canada (U.S. is 11th) (Munro, 2014; TCWF, 2014). First, these countries do not have to serve as many people as does the U.S. Based on population, the U.S. currently has approximately 320,051,000 people, compared to the U.K. which has 63,136,000, Australia with 23,343,000, France with 64,291,000, Germany with 82,727,000, and Canada with 35,182,000 (Potyra, 2016). It is easier to manage a smaller amount of people compared with a larger group, hence other countries appear better per capita in the accessibility and delivery of healthcare. The most current figures demonstrate that approximately 223 million people in the U.S. have private health insurance, 60.48 million have public insurance, while only 12.8% of the population do not have insurance (CDC, 2015). These figures alone exceed the population of most of the countries by which the U.S. is being compared to, meaning that the U.S. is providing healthcare to more people than most of the other countries.
There is no argument that the U.S. is one of the richest countries in the world. Based on the size of economy, or gross domestic product (GDP), the U.S. ranks first compared to the other countries with approximately $18.5 – 19 trillion (Knoema, 2016; Bergmann & Yellin CNN, 2016). The other countries that rank higher in healthcare have significantly less GDPs, with Germany having $3.5 trillion, U.K with $3 trillion, and Canada with $1.7 trillion to name a few (Bergmann & Yellin CNN, 2016). In healthcare expenditures, the U.S. spends 17.1% of its total GDP, while the rest of the countries, that are being compared with the U.S. as having better healthcare, spend approximately nine to almost 12% of their national GDP on healthcare (TCWF, 2013). What this indicates is that the U.S. has to spend more of its money on healthcare because they have to pay for more people to receive quality healthcare while at the same time attempting to maintain financial stability within the country. Financial stability is important in a country because it measures how comfortable people are living in the country. The U.S. has the highest disposable individual income with an average of $41,071 a year, as opposed to the average individual income of people in the comparison countries who only have an income average of approximately $29,016 (OECD, 2015; Willet, 2013). This means that the average American who needs to spend money on healthcare is more financially stable compared to those living within the other comparing countries who supposedly are being reported to have better healthcare than the U.S.
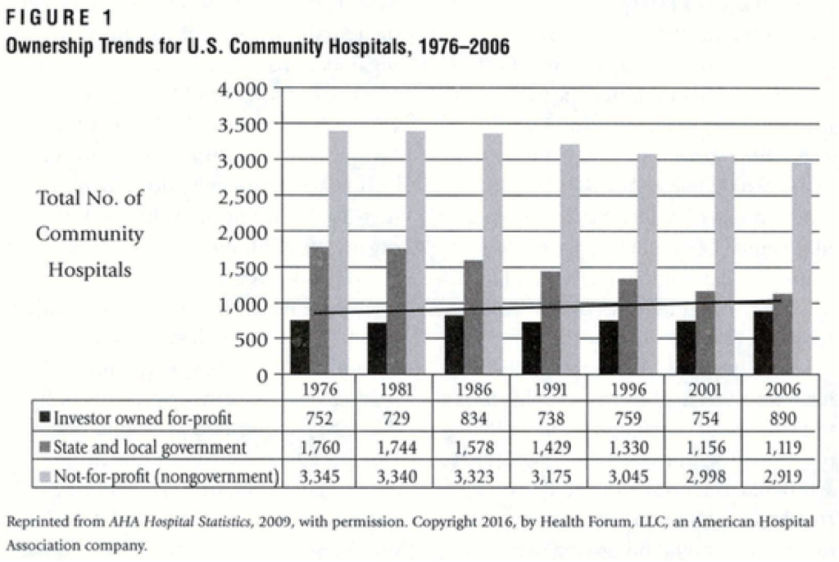
Another financial reason as to why the U.S. has a higher healthcare expenditure is based on the nature of how healthcare is being paid for currently. Managed care is the most common method of how healthcare is paid for in the U.S. The basic principle of managed care is a patient is enrolled with an insurance provider (commercial like Humana, government like Medicaid, or both) in which the patient pays an agreed periodic payment plan of monthly or quarterly, with premium payments such as co-pay (a set amount of money that a patient pays for a medical service) or yearly fees (Wahi, 2013; ereflect, 2009), also known as capitation. The patient benefits from the insurance provider by receiving discounted medical fees that the insurance provider has negotiated with a medical facility (Gapenski & Pink, 2007; Wahi, 2013). Those without an insurance provider have to pay an out of pocket upfront cost for the rendered care / service they will and / or have received based on the charges that a medical facility has determined are appropriate according to the local, regional, or national market value (Wahi, 2013; Gapenski & Pink, 2007). Since the insurance providers negotiate discounted prices for medical services it now makes profit margins small, meaning hospitals and clinics and medical facilities do not make a large amount of money in the delivery of healthcare; they barely make enough to stay operational (Evans et al., 2016). The lasting affect of this system is expensive healthcare.
Furthermore, the U.S. currently has the Affordable Care Act (ACA) which currently is being implicated as a factor that is making healthcare more expensive. A major contributing factor is that it mandate that every individual who applies for health insurance will be accepted regardless of what medical condition(s) they currently have, and the ACA does not allow for insurance providers to screen for which patient(s) they want to pay for their medical care (Hood, 2014; Yogada et al., 2014). Since everyone is being accepted without restrictions, insurance providers and medical facilities now needed to increase their medical care prices in order to meet the increase demand and to cover everyone who shows up on their doorstep (Hood, 2014). The increase in costs were evident as far back as 2010 when healthcare costs increased by ten percent. Today healthcare costs are estimated to increase by as much as 60% within the next several years (Hood, 2014). The ACA legislation also increased the amount of upfront costs required from patients before an insurance company will pay for the rest of the medical bill. Currently these upfront costs range from $5,000 to as much as $10,000 for major medical expenses such as surgeries (Hood, 2014). These are a couple of the major reasons as to why healthcare is expensive for people in the U.S. Also it should be mentioned that the current well- being of the U.S. population does not help reduce any of the healthcare costs as well.
The current health status of the people in the U.S. is dismal. We have the worst healthiest population in the world in terms of contracting preventable diseases, which are obesity and chronic diseases. The rate of adult obesity is 33.7% (ProCon, 2016), and 20% in children (Hood, 2014). In dollar figures, in 2009-2010, $160 billion was spent on treating health issues in people that were attributable to obesity. The costs of the ailments, which develop related to obesity, is about $150,976 up to as much as $301,952 more a year as compared to a healthy person (Hood, 2014). This is a great deal because obesity leads to chronic diseases such as strokes, diabetes, and cancer. This explains why it equates to spending so much more money on treating these individuals as it would to keep as person healthy (Hood, 2014). With so many unhealthy people, it is no wonder healthcare per person is about $9,523 per person a year (Fox, 2016), but this does not mean that healthcare quality is the worst as compared to other countries mentioned earlier in this report.
U.S. and Healthcare: National and International Views
Superficially looking at U.S. healthcare, the country does not look good. Currently the U.S. ranks 11th out of all the other ten countries previously mentioned based on four out of 11 criteria with ranking no better than 3rd. The ranking criteria were established by the World Health Organization (WHO), and the Organization for Economic Cooperation and Development (OECD) (TCWF, 2014). The U.S. was ranked 11th in cost-related problems, efficiency, equity, and healthy lives. Also the U.S. received an overall ranking of 11th based on the entire healthcare related data that was collected in 2013 (TCWF, 2014). The two highest ranking countries were the U.K. and Switzerland and the two lowest ranking countries were Canada and the U.S. (TCWF, 2014). Fortunately, this does not mean that the U.S. has the worst healthcare in the world.
The U.S. most assurdly understands the importance of healthcare deliverance, hence it ranks number one in healthcare expenditures with 17.1% of the GDP going towards healthcare costs (TCWF, 2015; OECD, 2015). This means that the U.S. wants to take care of its people no matter the costs. Also, even though the U.S. was evaluated based on healthcare data collection, data collections are not fully accurate, though they represent a general idea, they can also present an inaccurate depiction of the atmosphere of the U.S. healthcare. Healthcare practice in the U.S. is based on evidence-based practice, vetted by scientific method research studies that are repeatable to increase their validity (Claxton et. al, 2015). Also, the oversight of healthcare is managed by highly respectable, recognizable, professional organizations committed to the annual improvement of healthcare in the U.S. Professional organizations committed to this improvement in healthcare include, but not limited to: WHO, OECD, National Quality Forum, Agency for Healthcare Research and Quality (AHRQ), The Centers for Medicare and Medicaid Services (CMS), Institute of Medicine (Claxton et al., 2015). These organizations work with the government and medical providing facilities (both for-profit and non-profit) to improve healthcare. Over the years the U.S. has steadily improved in the deliverance, quality and accessibility of medical care. With so many organizations helping the U.S. to properly change its healthcare system it is no doubt that it takes time before positive effects are seen for patients.
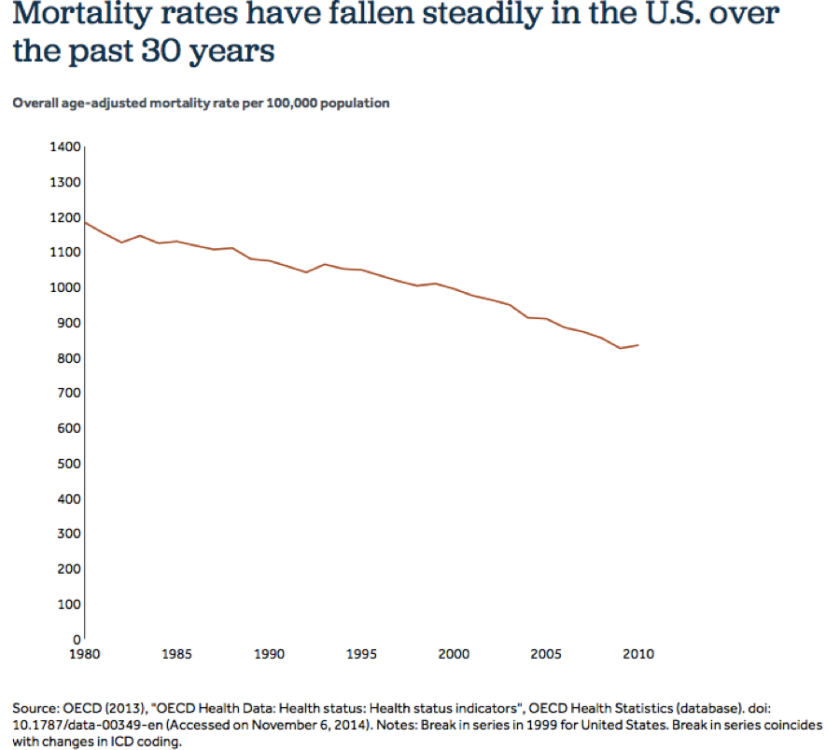
In the past three decades, the U.S. has made advances in over 20 medical outcomes. Most notable ones are mortality rate, resulting from 96 per 100,000 patients in 2004-05, to 86 per 100,000 (Claxton et al., 2015). From 1990 to 2010, pre-mature deaths and changes in poor health status improved by 14%. The number of individuals indicating as being in an excellent health status was also reported to be 19%, but 18% reported fair or poor health in 2013 (Claxton et al., 2015). Death rate in hospital admissions for strokes, heart attacks and pneumonia also showed positive improvements, with another 14% decrease rate of hospital acquired adverse conditions (bed ulcers, infections, drug interactions errors) (Claxton et al., 2015). Also notable was the reported number of amputations due to diabetes had decreased from 37.5 per 100,000 in 2006, to only 17.1 in 2010 (Claxton et al., 2015). There were also increases in patients receiving care who needed care with a rate change of 66% to 70% from 2005 to 2010 (Claxton et al., 2015). Also reported was an increase in the favorable outcomes, treatments and cures, of cancer in the U.S. had improved in the last decade as compared to that of other countries (Claxton et al., 2015). Overall, mortality rate in the U.S. went from 1200 per 100,000 to less than 850 per 100,000 over the span of 30 years, showing that the U.S. healthcare is steadily improving (Claxton et al., 2015).
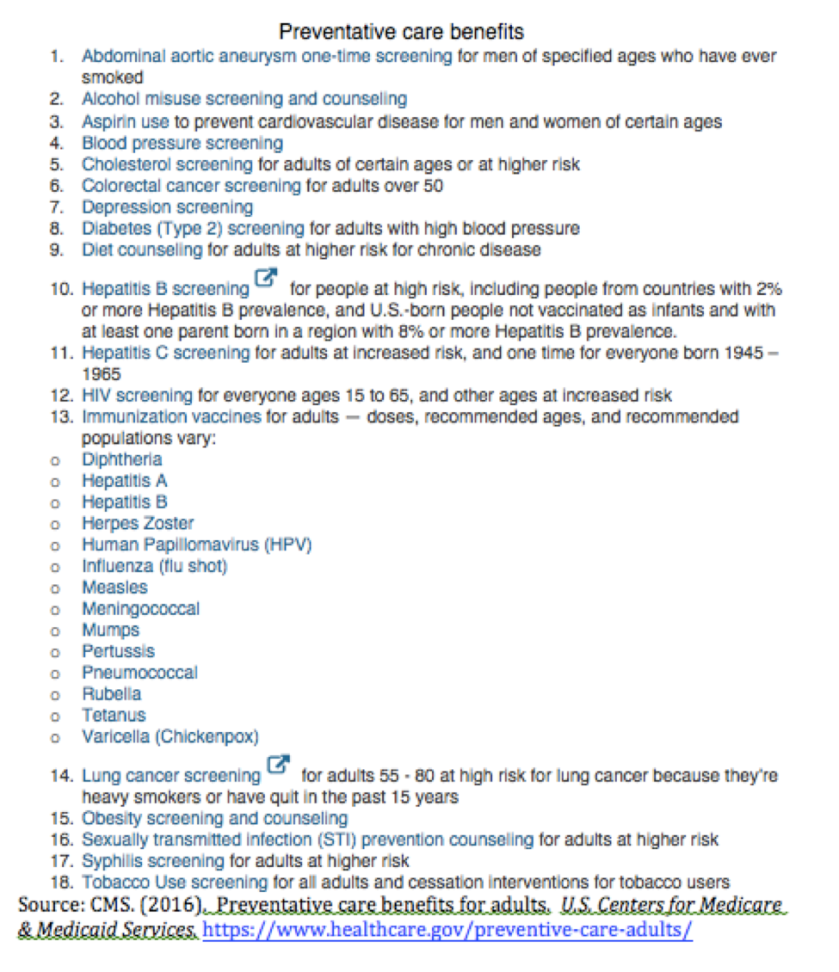
U.S. healthcare achieved another major improvement by including preventative care benefits in all insurance under Affordable Care Act. This allowed 18 preventative health and wellness screening tests to be involved in patients’ healthcare plan. Below is the specific tests that are included. This is a great achievement as more children and adults received important health essentials, especially vaccines and lab tests that detects early diseases and potentially prevent them from becoming chronic diseases (Claxton et al., 2015).
Earlier, it was mentioned that U.S. not only has the largest population compared to all the other nations by which it is being compared, but also has the largest number of unhealthiest people as well. Such challenges contribute to the U.S. having some of the worst medical outcomes as compared to the other nations previously mentioned. The more people who are difficult to medically manage the poorer the overall outcomes will be as compared to the other less numbers of people in other nations. Also another contributing factor for poor healthcare outcomes and unhealthy individuals is related to the declining number of physical education classes given in schools across this nation. The U.S. needs to increase active participation and numbers of gym classes that are offered in schools as well as place an increase emphasis on health education, making it mandatory to implement health classes across all education levels up to senior year of high school. As mentioned previously the U.S. is leading the way in the incidence of obesity in its population. This again relates to the importance that physical fitness and health education classes should be an integral part of each grade level in primary and secondary schools. Internationally, all the other countries faired better than the U.S. in critical aspects of medical care such as overall mortality rate, diabetes rates, hospital admissions, and wait times for acute care visits (Claxton et al., 2015). Together these results make sense based on the fact that the nation with the unhealthiest population was the U.S. based on a variety of healthcare data collected and why we were ranked as number 11 out of the most richest countries. Again keeping in mind that we have the most population to take care of, the U.S. healthcare system did show improvements overtime. Such improvements are a positive outlook for the future of U.S. healthcare.
Conclusion
It is clear that U.S. healthcare looks to be behind ten other of the richest countries in the world. This is with good reasons, these include that the U.S. has the greatest population to take care of who are the unhealthiest in the world and a pay system that does not increase profit margins for medical facilities. These contribute to the increasing price of healthcare. Fortunately, the U.S. does most assurdly show that they have made gains over time, and with the help of the government and medical organizations more improvements will come. Before criticizing how awful the U.S. healthcare system is, one must first be educated with what the U.S. has to deal with, then venture another judgment, because there are far worst places in the world that have far less quality and accessibility of healthcare. Lastly one should also realize that they will make more money in the U.S. than those other countries so they (you) can afford healthcare in this country.
Reference
Bergmann, A., Yellin, T. (2016). World’s largest economies. Cable News Network. A Time Warner Company, CNN Money. Retrieved from http://money.cnn.com/news/economy/world_economies_gdp/
Claxton, G., Cox, C., Gonzales, S., Kamal, R., Levitt, L. (2015). Measuring the quality of healthcare in the U.S. Kaiser Family Foundation, Peterson-Kaiser Health System Tracker, Insight Brief, p1. http://www.healthsystemtracker.org/insight/measuring-the-quality-of-healthcare-in-the-u-s/
CDC. (2015). Health insurance coverage. Centers for Disease Control and Prevention, U.S. Department of Health & Human Services, p.1. https://www.cdc.gov/nchs/fastats/health-insurance.htm
CMS. (2016). Preventative care benefits for adults. U.S. Centers for Medicare & Medicaid Services. https://www.healthcare.gov/preventive-care-adults/
ereflect. (2009, November 16). What does managed care mean[Video file].http://www.youtube.com/watch?v=ipkKEScKuRM
Evans, D.V., CawseLucas, J, Ruiz, D.R., Allcut, E.A., Andrilla, H.A., & Norris, T. (2016). Family medicine resident billing and lost revenue: A regional crosssectional study. Department of Family Medicine from Univ of Washington and PeaceHealth Southwest Medical Center 47(3). http://www.stfm.org/FamilyMedicine/Vol47Issue3/Evans175
Fox, M. (2016). United States comes in last again on health, compared to other countries. NBC News, Health, Health Care. Retrieved from http://www.nbcnews.com/health/health-care/united-states-comes-last-again-health-compared-other-countries-n684851
Gapenski, L.C. & Pink, G.H. (2007). Understanding healthcare financial management. Retrieved from http://www.ache.org/pubs/chap1-3gapenski5th.pdf
Hawkins-Hood (Presenter), Healthy Learning (Producer), (2014). Health reform update: Wellness is the key [Video file].http://proxy1.ncu.edu/login?url=https://search.alexanderstreet.com/avon/view/work/3211122
Knoema. (2016). World GDP ranking 2016 | data and charts | forecast. Knoema, Economy, GDP, World Rankings. https://knoema.com/nwnfkne/world-gdp-ranking-2016-data-and-charts-forecast
Munro, D. (2014). U.S. healthcare ranked dead last compared to 10 other countries. Forbes. Retrieved from http://www.forbes.com/sites/danmunro/2014/06/16/u-s-healthcare-ranked-dead-last-compared-to-10-other-countries/#310634701b96
OECD. (2015). United States. Organization for Economic Cooperation and Development, Better Life Index, p. 1. http://www.oecdbetterlifeindex.org/countries/united-states/
ProCon. (2016). Global obesity levels. ProCon.org, nonprofit public charity. http://obesity.procon.org/view.resource.php?resourceID=006032
Potyraj, J. (2016). The quality of US healthcare compared with the world. American Journal of Managed Care, p. 1. http://www.ajmc.com/contributor/julie-potyraj/2016/02/the-quality-of-us-healthcare-compared-with-the-world
TCWF. (2013). U.S. health care from a global perspective. THE COMMONWEALTH FUND, Publications, Issue Briefs, p.1. http://www.commonwealthfund.org/publications/issue-briefs/2015/oct/us-health-care-from-a-global-perspective
TCWF. (2014). Mirror, mirror on the wall, 2014 update: how the U.S. health care system compares internationally. THE COMMONWEALTH FUND, Publications, Fund Reports, p. 1 http://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirror-mirror
Wahi, M. (2013, May 26). Major characteristics of the u.s. health care system. [Part 1] [Video File][Power Point Presentation]. Retrieved from https://www.youtube.com/watch?v=HA2tsmxiFAE
Willet, M. (2013). The 15 countries with the highest quality of life. Business Insider, Inc. Retrieved from http://www.businessinsider.com/top-countries-on-oecd-better-life-index-2013-5#
Yagoda, L., Duritz, N., & Friedman, J. (2014). Affordable Care Act for dummies cheat sheet. Dummies A Wiley Brand. Retrieved from http://www.dummies.com/health/affordable-care-act-for-dummies-cheat-sheet/
For needed corrections, contact j.serrano5422@email.ncu.edu